

From ATLAS OF SKULL BASE SURGERY & NEUROTOLOGY. Thieme. ©2009
All images are copyright by RK Jackler. Permission granted for non-profit educational use of images, with attribution to their source.
Created by: Robert Jackler (surgeon) and Christine Gralapp (artist).
With contributions by:
Nikolas Blevins, Griffith Harsh, Michael Kaplan, Lawrence Pitts, Charles Yingling, and Corey Mass.
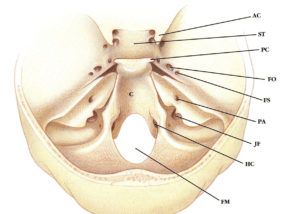
For legend references, please see the print book.